



Sulfur is called nature's "beauty mineral" because it keeps skin smooth and youthful and hair glossy. Sulfur is necessary for the production of collagen and keratin, proteins necessary for the health and maintenance of skin, nails and hair'
$14.95

Iodine is a trace mineral that is vital to the function of the thyroid gland. The human body does not make iodine, so all iodine intake must come from either our diet or from supplements.
|
|
Cancer: >
Sarcoma
 SarcomaA sarcoma is a cancer that arises from transformed cells of mesenchymal (connective tissue) origin.[1][2] Connective tissue is a broad term that includes bone, cartilage, fat, vascular, or hematopoietic tissues, and sarcomas can arise in any of these types of tissues.[2][3] As a result, there are many subtypes of sarcoma, which are classified based on the specific tissue and type of cell from which the tumor originates.[4] It is important to note that sarcomas are primary connective tissue tumors, meaning that they arise in connective tissues.[2] This is in contrast to secondary (or "metastatic") connective tissue tumors, which occur when a cancer from elsewhere in the body (such as the lungs, breast tissue or prostate) spreads to the connective tissue.[5] The word sarcoma is derived from the Greek σάρξ sarx meaning "flesh".[6] ClassificationSarcomas are typically divided into two major groups: bone sarcomas and soft tissue sarcomas,[2] each of which has multiple subtypes. In the United States, the American Joint Committee on Cancer (AJCC) publishes guidelines that classify the subtypes of sarcoma.[4] These subtypes are as follows: Subtypes of bone sarcoma:
Subtypes of soft tissue sarcoma:
Signs and symptomsSymptoms of bone sarcomas typically include bone pain, especially at night, and swelling around the site of the tumor.[2] Symptoms of soft tissue sarcomas vary, but often present as firm, painless lumps or nodules.[2] Gastrointestinal stromal tumors (a subtype of soft tissue sarcoma) often are asymptomatic, but can be associated with vague complaints of abdominal pain, a feeling of fullness, or other signs of intestinal obstruction.[2] CauseCauses and risk factorsThe cause of most bone sarcomas is not known,[3] but several factors are associated with an increased risk of developing bone sarcoma. Previous exposure to ionizing radiation (such as prior radiation therapy) is one such risk factor.[2] Exposure to alkylating agents, such as those found in certain cancer chemotherapeutic medicines, also increases the risk of bone sarcoma.[3] Certain inherited genetic syndromes, including Li-Fraumeni syndrome, heritable RB1 gene mutations, and Paget's disease of bone, are associated with an increased risk of developing bone sarcomas.[2] Most soft tissue sarcomas arise from what doctors call "sporadic" (or random) genetic mutations within an affected person's cells.[3] Nevertheless, there are certain risk factors associated with an increased risk of developing soft tissue sarcoma. Previous exposure to ionizing radiation is one such risk factor.[2] Exposure to vinyl chloride (e.g., such as the fumes encountered in the production of polyethylene vinyl chloride (PVC)), arsenic and thorotrast all are associated with an increased risk of angiosarcoma.[2][3] Lymphedema, such as that resulting from certain types of breast cancer treatment, also is a risk factor for development of angiosarcoma.[3] As with bone sarcomas, certain inherited genetic syndromes also are associated with an increased risk of developing soft tissue sarcoma, including Li-Fraumeni syndrome, familial adenomatous polyposis, neurofibromatosis type 1, and heritable RB1 gene mutations.[3] MechanismsThe mechanisms by which healthy cells transform into cancer cells are described in detail elsewhere (see Cancer main page; Carcinogenesis main page). The precise molecular changes that result in sarcoma are not always known, but certain types of sarcomas are associated with particular genetic mutations.[2][3] Examples include:
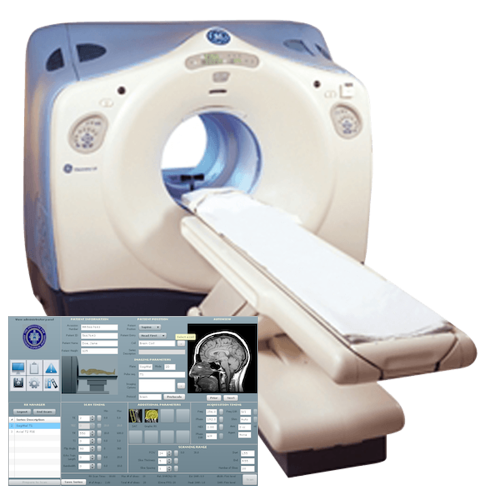
DiagnosisDiagnosis of bone sarcomas begins with a thorough history and physical examination which may reveal characteristic signs and symptoms (see Signs and Symptoms above).[3] Laboratory studies are not particularly useful in diagnosis, although some bone sarcomas (such as osteosarcoma) may be associated with elevated alkaline phosphatase levels, while others (such as Ewing Sarcoma) can be associated with elevated erythrocyte sedimentation rate.[7] Importantly, however, none of these laboratory findings are specific to bone sarcomas, meaning that elevations in these lab values are associated with many other conditions as well as sarcoma, and thus cannot be relied upon to conclusively diagnose sarcoma.[3] Imaging studies are critically important in diagnosis, and most clinicians will order a plain radiograph (X-ray) initially.[3] Other imaging studies commonly used in diagnosis include magnetic resonance imaging (MRI) studies and radioisotope bone scans.[7][3] Computed tomography (CT) imaging typically is not used in diagnosis of most types of bone sarcoma, although it is an important tool for staging (see below).[3] Definitive diagnosis requires biopsy of the tumor and careful review of the biopsy specimen by an experienced pathologist.[3] Diagnosis of soft tissue sarcomas also begins with a thorough history and physical examination.[3] Imaging studies can include either CT or MRI, although CT tends to be preferred for soft tissue sarcomas located in the thorax, abdomen, or retroperitoneum.[3] Positron emission tomography (PET) also may be useful in diagnosis, although its most common use is for staging (see below).[3]As with bone sarcomas, definitive diagnosis requires biopsy of the tumor with evaluation of histology by a trained pathologist.[3] StagingIn general, cancer staging refers to how advanced a cancer is, and usually it is based upon factors such as tumor size and whether it has spread to other parts of the body.[3][8] Staging is important because the stage affects the prognosis (likely outcome for the patient), as well as the types of treatments that are likely to be effective against the cancer.[2][4] With sarcomas, staging requires a determination of whether the tumor has grown into surrounding tissues ("local invasion"), as well as imaging to determine whether it has spread (a process known as "metastasis") to lymph nodes (forming "nodal metastases") or to other tissues or organs in the body (forming "distant metastases").[4] The most common imaging tools used for staging bone sarcomas are MRI or CT to evaluate the primary tumor, contrast-enhanced CT of the chest to evaluate whether the cancer has spread (i.e., metastasized) to the lungs, and radioisotope bone scan to evaluate whether the cancer has spread to other bones.[4] Staging for soft tissue sarcomas typically includes imaging of the primary tumor by MRI or CT to determine tumor size, as well as contrast-enhanced CT of the chest to evaluate for metastatic tumors in the lungs.[4] GradeLike some other cancers, sarcomas are assigned a grade (low, intermediate, or high) based on the appearance of the tumor cells under a microscope.[9] In general, grade refers to how aggressive the cancer is and how likely it is to spread to other parts of the body ("metastasize").[9] Low-grade sarcomas have a better prognosis than higher-grade sarcomas, and are usually treated surgically, although sometimes radiation therapy or chemotherapy are used.[3][4] Intermediate- and high-grade sarcomas are more frequently treated with a combination of surgery, chemotherapy, and/or radiation therapy.[10] Since high-grade tumors are more likely to undergo metastasis (invasion and spread to locoregional and distant sites), they are treated more aggressively. The recognition that many sarcomas are sensitive to chemotherapy has dramatically improved the survival of patients. For example, in the era before chemotherapy, long-term survival for pediatric patients with localized osteosarcoma was only about 20%, but now has risen to 60–70%.[11] Prevention and screeningIn the US, the US Preventative Services Task Force (USPSTF) publishes guidelines recommending preventative screening for certain types of common cancers and other diseases.[12] As of March 2019, the USPSTF does not recommend screening for sarcoma,[12] possibly because it is a very rare type of cancer (see Epidemiology below). The American Cancer Society (ACS) also publishes guidelines recommending preventative screening for certain types of common cancers.[13] Like the USPSTF, as of March 2019 ACS does not recommend preventative screening for sarcoma.[13] TreatmentSurgery is the most common form of the treatment for most sarcomas that have not spread to other parts of the body.[3][14] Limb-sparing surgery, as opposed to amputation, can now be used to save the limbs of patients in at least 90% of extremity (arm or leg) sarcoma cases.[14] Additional treatments, including chemotherapy and radiation therapy (also called "radiotherapy"), may be administered before surgery (called "neoadjuvant" chemotherapy or radiotherapy) and/or after surgery (called "adjuvant" chemotherapy or radiotherapy).[3][10] The use of neoadjuvant or adjuvant chemotherapy and radiotherapy significantly improves the prognosis for many sarcoma patients.[3][15] Treatment can be a long and arduous process, lasting about a year for many patients.[10]
Expression of receptor B7-H3 provides a promising target for new immunotherapeutic strategies. PrognosisFactors that affect prognosisThe AJCC has identified several factors that affect prognosis of bone sarcomas:[4]
For soft tissue sarcomas other than GISTs, factors that affect prognosis include:[4]
For GISTs, the key factor that affects prognosis is:[4]
Outcome dataAccording data published by the US National Cancer Institute (NCI), the overall 5-year for survival for bone sarcomas is 66.9%.[20] The American Cancer Society (ACS) estimates that 1,660 people in the US will die in 2019 from bone sarcomas, accounting for 0.3% of all cancer deaths.[21] The median age at death is 61 years old, although death can occur in any age group.[20] Thus, 12.3% of bone sarcoma deaths occur in people under 20 years old, 13.8% occur in people 20-34 years old, 5.5% occur in people 35-44 years old, 9.3% occur in people 45-54 years old, 13.5% occur in people 55-64 years old, 16.2% occur in people 65-74 years old, 16.4% occur in people 75-84 years old, and 13.1% occur in people 85 years or older.[20] For soft tissue sarcomas, the overall 5-year survival (irrespective of stage) is 64.5%, but survival is affected by many factors, including stage.[22] Thus, the 5-year survival is 80.8% for soft tissue sarcomas that have not spread beyond the primary tumor ("localized" tumors), 58.0% for soft tissue sarcomas that have spread only to nearby lymph nodes, and 16.4% for soft tissue sarcomas that have spread to distant organs.[22] The ACS estimates that 5,270 people will die from soft tissue sarcoma in 2019, accounting for 0.9% of all cancer deaths.[21] EpidemiologySarcomas are quite rare.[2] The risk of a previously healthy person receiving a new diagnosis of bone cancer is less than 0.001%, while the risk of receiving a new diagnosis of soft tissue sarcoma is between 0.0014-0.005%.[3] The American Cancer Society estimates that in the United States there will be 3,500 new cases of bone sarcoma in 2019, and 12,750 new cases of soft tissue sarcoma.[21] Considering that the total estimated number of new cancer diagnoses (all types of cancer) is 1,762,450, this means bone sarcomas represent only 0.2% of all new cancer diagnoses (making them the 30th most common type of cancer[20]) and soft tissue sarcomas represent only 0.7% (making them the 22nd most common type of cancer[22]) of all new cancer diagnoses in the US in 2019.[21] These estimates are similar to previously reported data.[3] Sarcomas affect people of all ages. Around 50% of bone sarcomas and 20% of soft-tissue sarcomas are diagnosed in people under the age of 35.[23] Some sarcomas, such as leiomyosarcoma, chondrosarcoma, and gastrointestinal stromal tumor (GIST), are more common in adults than in children.[2] Most high-grade bone sarcomas, including Ewing's sarcoma and osteosarcoma, are much more common in children and young adults.[2] ResearchTreatment of sarcoma, especially when the sarcoma has spread, or "metastasized", often requires chemotherapy but existing chemotherapeutic medicines are associated with significant toxicities and are not highly effective in killing cancer cells.[3] Therefore, research to identify new medications to treat sarcoma is bing conducted as of 2019.[3] One possibility is the use of cancer immunotherapy (e.g., immune checkpoint inhibitors like anti-PD1, anti-PDL1, and anti-CTLA4 agents) to treat sarcomas.[25] This is not yet an established treatment tool.[25] Other strategies, such as small-molecule targeted therapy, biologic agents (e.g., small interfering RNA molecules), and nanoparticle-directed therapy, also are being investigated.[3] Research to understand the specific genetic and molecular factors that cause sarcoma to develop is underway.[3] This could allow for the design of new targeted therapies and allow physicians to more accurately predict a patient's prognosis.[3] Presence of the H3-B3 immunoregulatory checkpoint receptor in the tumor cells provides the opportunity for clinical trial testing of new drugs and targeted agents and immunotherapies in development. AwarenessIn the US, July is widely recognized as Sarcoma Awareness Month.[26] The UK has a Sarcoma Awareness Week in July led by Sarcoma UK, the bone and soft-tissue cancer charity.[27] References
|
|
|

OPEN 24 HOURS: ACCIDENT EMERGENCY, LAB SERVICES, IMAGING SERVICES & PHARMACY


Medical Disclaimer: The Contents of this site is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or treatment.


Medical Disclaimer: The Contents of this site is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or treatment.